Objective: Punch biopsy is a simple and effective diagnostic technique used in hard-to-heal wound management. Histologic examination can rule out cancer in the wound bed or diagnose vasculitis in a hard-to-heal or suspicious ulcer. A biopsy can determine the level of bacteria in an ulcer when infection is suspected. Despite its use, health professionals practicing in wound clinics hesitate to perform punch biopsies. The reasons vary from the invasive nature of the procedure to a fear of complications.
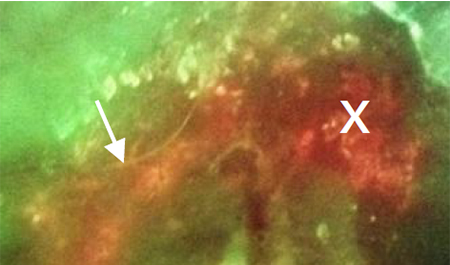
Methods: A multicentre clinical trial evaluated the addition of fluorescence imaging (MolecuLight i:X) to clinical examination in determining bacterial burden in hard-to-heal wounds. The protocol required a 6mm punch biopsy of any area (up to three) suspected of having moderate-to-high bacteria levels either on clinical examination or fluorescence image. If clinical examination and fluorescence imaging both did not indicate bacteria, the health professional took a biopsy of the centre of the ulcer. The biopsies were performed under local anaesthesia after cleansing the ulcer bed with sterile normal saline. Haemostasis was achieved with direct pressure and the occasional topical clotting agent. All of the patients were followed for 30 days to monitor for adverse events.
Results: A total of 350 patient’s with wounds (diabetic foot ulcer n=138; venous leg ulcer n=106; pressure ulcer n=22; surgical site infection n=60; other n=24), enrolled by 20 investigators at 14 sites in the US, underwent a total of 412 punch biopsies. Haemostasis was achieved in all 412 biopsies. No biopsy sites required cautery or suture ligation to control bleeding. No subjects returned to the clinic secondary to bleeding. A patient developed an infection three days post-biopsy that could have been due to the punch biopsy. However, the patient was HIV-positive and the quantitative biopsy was positive for infection, biopsy bacterial load of 106 colony forming units (CFU)/g.
Conclusion: This trial used a 6mm punch to obtain tissue for culture, histology and additional biomarker research. In daily wound care practice, a smaller 3mm punch suffices. Adverse events were rare despite the larger biopsy. Punch biopsies are a safe procedure for obtaining tissue for histologic or microbiologic analysis.
NOTE: All real-time fluorescence imaging in this trial was performed using the MolecuLight i:X® real-time imaging device for bacterial detection and digital wound measurement.