Back to All Clinical Evidence
![]()
![]()
![]()
![]()
![]()
![]()
![]()
 PUBLICATION_
PUBLICATION_  PUBLICATION_
PUBLICATION_ 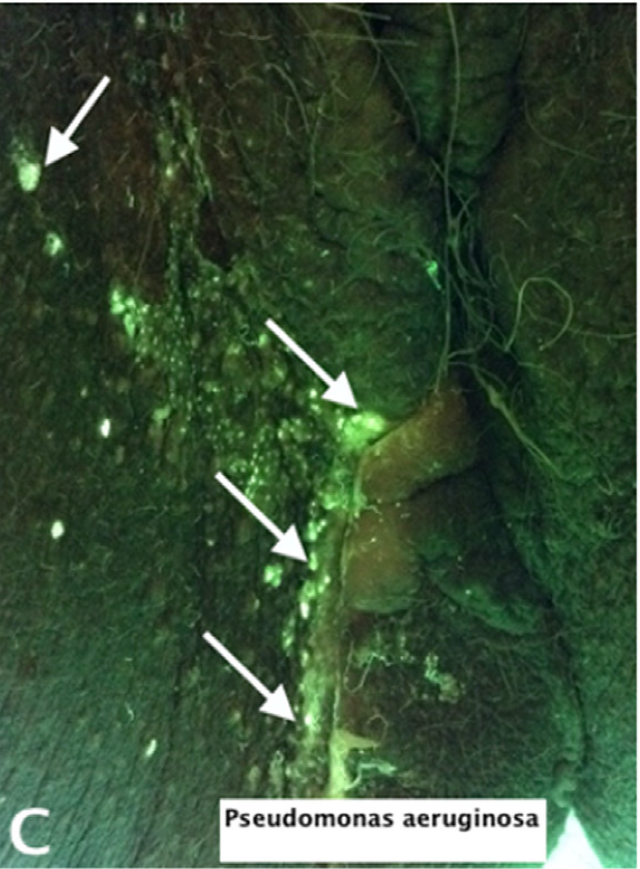 PUBLICATION_
PUBLICATION_ 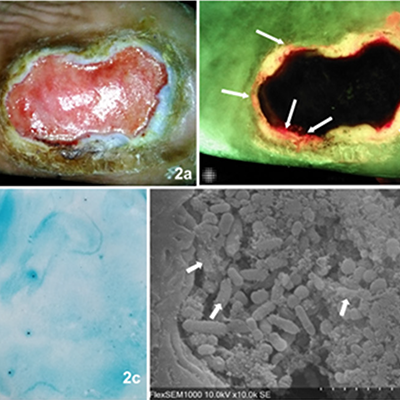 PUBLICATION_
PUBLICATION_
Accelerated Wound Healing, Accelerated Wound Healing
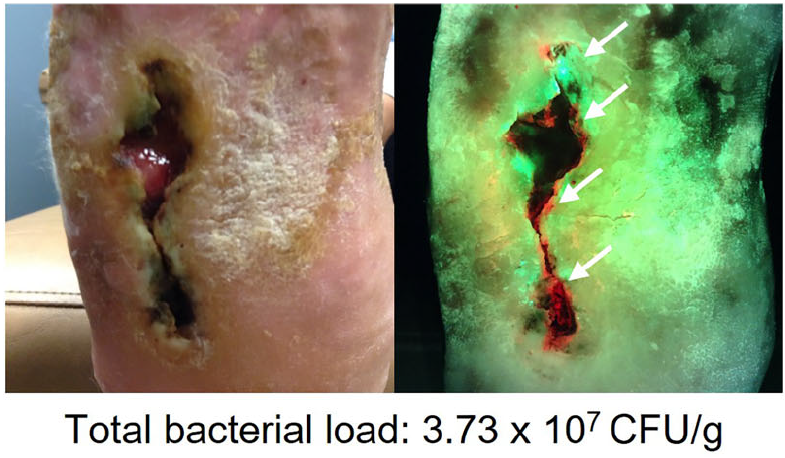
Use of a bacterial fluorescence imaging device: wound measurement, bacterial detection, and targeted debridement
PUBLICATION_ Uncovering the high prevalence of bacterial burden in surgical site wounds with point-of-care fluorescence imaging
PUBLICATION_ Integrating Point-of-Care Bacterial Fluorescence Imaging-Guided Care with Continued Wound Measurement for Enhanced Wound Area Reduction Monitoring
PUBLICATION_ Bacterial autofluorescence in infected perineal wounds: A prospective cohort study
PUBLICATION_ Assessing Biofilm at the Bedside: Exploring Reliable Accessible Biofilm Detection Methods
Ready to see the difference?


MolecuLight is SOC ll®
Type l Accredited:

MolecuLight awarded
Premier’s
Technology
Breakthrough Designation

MolecuLight
i:X
is designated as a:

MolecuLight included
in ISWCAP Consensus
Guidelines:
MolecuLight is a proud
corporate member of:
Global
USA
©2026
The MolecuLight® i:X and MolecuLightDX™ Imaging Devices are approved by Health Canada for sale in Canada and has CE marking for sale in the European Union.
The MolecuLight™ i:X and DX Imaging Devices have received FDA clearance.